
I have been involved continuously in basic cellular and molecular transplant immunology for 30 years and have been continuously funded for the entire time. My basic research has always focused on T cell immunobiology, and for more than 20 years has also focused on issues of migration, trafficking, secondary lymphoid organ structure and function, and lymphatic structure and function, and how these processes and structures influence T cell immunity and T cell tolerance in models of transplantation. I have also maintained an active clinical practice in solid organ transplantation and am thus constantly exposed to the problems of patients and their immune systems, including cellular and humoral rejection, opportunistic infections, chronic viral disease, autoimmune organ failure, and immunosuppression medication side effects. I have had over 60 trainees in my lab, am actively involved in teaching and mentoring.
I. Cellular and Molecular Immunology and Lymph Node Structure
Regulatory T Cells and Lymphatic Endothelial Cells: Regulatory Interactions for Migration and Function
Our investigations unraveled the key signaling pathways controlling Treg migration. Thymus derived (nTreg) and peripherally induced Treg (iTreg) express high cell surface levels of lymphotoxin ab (LTab). Treg, but not Tconv, use LTab to migrate from grafts across afferent lymphatic endothelial cells (LEC) and into dLN. Treg LTab binds the LEC LTb-receptor (LTbR) to stimulate non-canonical NFkB-inducing kinase (NIK). NIK signaling facilitates Treg transendothelial migration (TEM) by inducing LEC responses, including increased CCL21 expression, VCAM-1 rearrangement, and increases in basal lamellipodia that engage Treg. Our new preliminary studies now show that Treg-LEC interactions: 1.) use LTab-LTbR to condition LEC for permissiveness for TEM; 2.) determine the transition of Treg to become exTreg; and 3.) rely on Treg PD-1 and LEC PD-L1 TEM. Our data demonstrate novel Treg-LEC interactions that serve essential roles for Treg suppression and identify unique therapeutic opportunities for modulating immunity.
Sponsor: NIH – National Institutes of Health
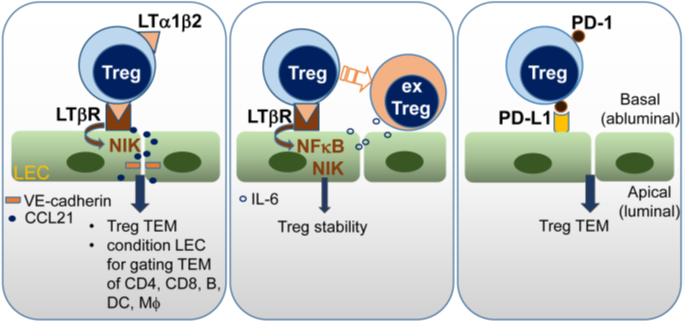
Treg-LEC are a regulatory nidus for suppression and tolerance. 1.) LTab-LTbR interactions condition the permissiveness of LEC for gating TEM of other leukocyte subsets. 2.) Treg-LEC interactions determine if Treg maintain suppressive functions or become exTreg. 3.) TEM relies on a novel role for PD-1-PD-L1.
Regulatory T Cells Condition Lymphatic Endothelia for Enhanced Transendothelial Migration. Piao W, Xiong Y, Li L, Saxena V, Smith KD, Hippen KL, Paluskievicz C, Willsonshirkey M, Blazar BR, Abdi R, Bromberg JS. Cell Rep. 2020 Jan 28;30(4):1052-1062.e5. doi: 10.1016/j.celrep.2019.12.083.
Lymph Node Structure and Function in Tolerance: Role of Laminins
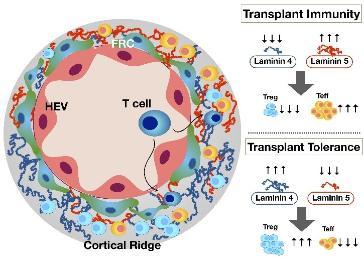
Our new data indicate that stromal cells regulate the LN laminin a4:a5 ratio and control the fate of the immune response toward inflammation and immunity (low ratio) or toward suppression and tolerance (high ratio). Our specific hypothesis is that LN stromal cells integrate immune cues and thus regulate laminin structures, and this integration is a final common pathway that channels the immune response and allograft outcomes. The corollaries are: 1) laminins regulate the response to inflammation and immunity, which results in pro-inflammatory LN structures or even the pathologic response of immunologic scarring; and 2) laminins regulate the response to suppression and tolerance and result in homeostatic and pro-tolerogenic LN structures.
Sponsor: NIH – National Institutes of Health
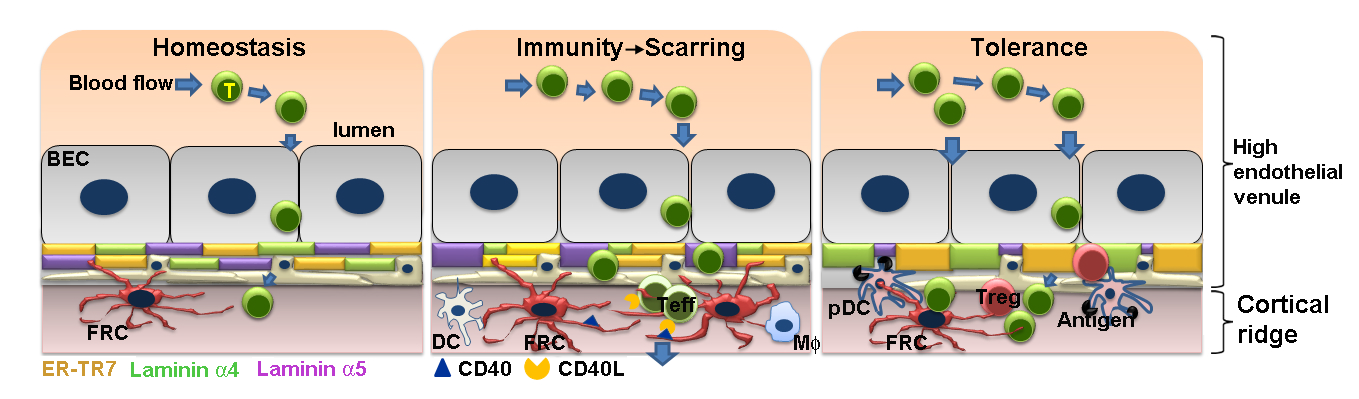 Figure 1. Model for Specific Aims. Differential expression of laminins regulates T cell migration in HEV and CR, iTreg induction, and T cell suppression, determining tolerance vs. immunity. Stromal cells such as FRC integrate the immune cues of inflammation and immunity by regulating LN laminin structure, and this integration is a final common pathway that channels the immune response and outcomes.
Figure 1. Model for Specific Aims. Differential expression of laminins regulates T cell migration in HEV and CR, iTreg induction, and T cell suppression, determining tolerance vs. immunity. Stromal cells such as FRC integrate the immune cues of inflammation and immunity by regulating LN laminin structure, and this integration is a final common pathway that channels the immune response and outcomes.
Aim 1 - Demonstrate that pro-inflammatory LN structures promote inflammation to prevent tolerance.
Aim 2 - Define mechanisms of stromal cell responses.
Aim 3 – Define specific immunosuppression that results in LN structures that support tolerogenic immune responses.
The lymph node stromal laminin α5 shapes alloimmunity. Li L, Shirkey MW, Zhang T, Xiong Y, Piao W, Saxena V, Paluskievicz C, Lee Y, Toney N, Cerel BM, Li Q, Simon T, Smith KD, Hippen KL, Blazar BR, Abdi R, Bromberg JS. J Clin Invest. 2020 May 1;130(5):2602-2619. doi: 10.1172/JCI135099.
Immunological and Functional Consequences Triggered by the Gut Microbiota Regulate Alloimmunity and Cardiac Transplant Outcome
Many aspects of the innate and adaptive immunity are critically regulated by the microbiota. Microbial cells, their metabolites and nucleic acids engage various immune cells, resulting in pro- or anti-inflammatory signals that differ based on chemical structures, cellular receptors, and physiological context. The microbiota not only influences local immunity, but also has distant effects on systemic immunity. Local microbiota stimulation of innate and adaptive immune cells results in those cells or their products to migrate or traffic through lymphatics or blood, and influence diseases. Our results show that both pro-inflammatory and anti-inflammatory microbiota populations, as well as single bacteria, can be defined by their effects on the long-term outcome of the grafts. We hypothesize that the microbiota directly regulates innate immunity, which in turn regulates systemic inflammation and adaptive immunity, thereby determining the occurrence and progression of graft fibrosis, inflammation and graft survival. The definition of pro-inflammatory and anti-inflammatory microbiota and strains may provide a precise platform to define the most important upstream influences that initiate organ inflammation and scarring and could serve as potent diagnostic markers for allograft management.
Sponsor: NIH – National Heart, Lung, and Blood Institute
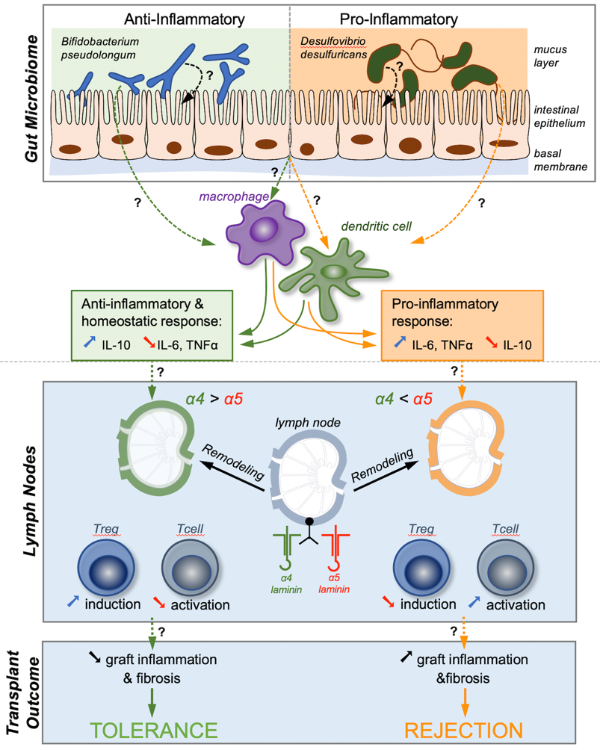
We have developed a general framework detailing the paths linking the gut microbiome to transplant outcome. Our results so far show that signals from selected species from the gut microbiome, such as the Bifidobacterium stimulates innate immunity cells, such as macrophages and dendritic cells, which influence LN laminin α4/α5 remodeling, alloantigen specific T cell fate, and allograft outcome.
Gut microbiota-dependent modulation of innate immunity and lymph node remodeling affects cardiac allograft outcomes. Bromberg JS, Hittle L, Xiong Y, Saxena V, Smyth EM, Li L, Zhang T, Wagner C, Fricke WF, Simon T, Brinkman CC, Mongodin EF. JCI Insight. 2020 Aug 6;5(15):e142528. doi: 10.1172/jci.insight.142528.
Lymph Nodes at the Crossroads of Allo-Immunity and Regulation
Organ transplantation remains a mainstay therapeutic strategy for patients with end organ diseases. One of the highest unmet needs to improve long-term transplant outcomes is devising more effective immune modulation. This requires innovative mechanistic studies of transplant alloimmunity. The lymph node (LN) is the quintessential organ of alloimmunity. Our overarching hypothesis is that manipulating the microenvironment of LNs will provide a unique opportunity to direct the alloimmune reaction towards an anti-inflammatory tolerance response. Our major goals are to understand the cellular and molecular mechanisms that govern the microanatomical adaptation of the LN during immune activation or tolerance induction, and to develop highly innovative therapeutic strategies that promote a regulatory LN microenvironment and result in immune tolerance. This PPG sets forth a platform for connecting two teams (Drs. Abdi and Bromberg) with complementary skills and expertise in LN alloimmune-biology. Project 1 will test the hypothesis that sustained activation of fibroblastic reticular cells (FRCs) of the LN during alloimmunity will result in FRC transformation to proinflammatory myofibroblasts creating an inflammatory milieu within the LN, which would further promote alloimmunity. Our corollary hypothesis is that restoration of the function of FRCs and microanatomy of the LNs will enhance their immunoregulatory function and promote tolerance. Project 2 will test the hypothesis that FRCs regulate the LN laminin a4:a5 (LAMA4/LAMA5) ratio and control the fate of the immune response. The ultimate goal of these well-integrated and highly synergistic Projects and Cores is to generate transformative mechanistic data, which will lay the groundwork for developing highly targeted and innovative therapeutic strategies for transplantation.
Sponsor: Pres. and Fellows of Harvard College dba Harvard University
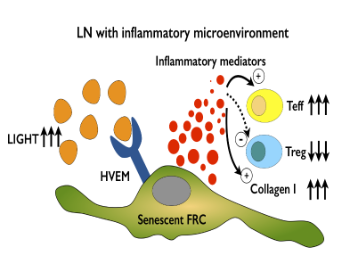
Project 1 will examine the function of the HVEM/LIGHT pathway in shifting the differentiation of FRCs into proinflammatory myofibroblasts in the fibrotic LN creating a heightened inflammatory microenvironment perpetuating transplant immunity. Synergy from Project 2 for this Aim will include determining whether the HVEM/LIGHT pathway also regulates the ratio of LAMA4/5 in the CR of LN and Treg trafficking. Project 2 will carry out large genomic studies to discover new genes and processes regulating the function of FRCs.
Lymph node fibroblastic reticular cells deposit fibrosis-associated collagen following organ transplantation. Li X, Zhao J, Kasinath V, Uehara M, Jiang L, Banouni N, McGrath MM, Ichimura T, Fiorina P, Lemos DR, Shin SR, Ware CF, Bromberg JS, Abdi R. J Clin Invest. 2020 Aug 3;130(8):4182-4194. doi: 10.1172/JCI136618.
II. Bioengineering for the Manipulation of Immunity
Programming Immune Function Through Modular Assembly of Polyionic Immune Signals
Therapeutic vaccines for autoimmune diseases could benefit from approaches which provide persistent delivery of drugs that can direct or modulate inflammatory or self-reactive effects of autoimmunity. In this proposal we present an approach for direct lymph node delivery of biodegradable particles loaded with antigens and tolerizing small molecules drugs. This strategy couples efficient, persistent delivery of bioactive cargo to key cells of the immune system that could induce anti-inflammatory or protective functions without significant side effects. Ultimately, this approach could contribute to new biomaterial-based approaches for therapeutic vaccines aimed at combating autoimmune disorders like multiple sclerosis.
Sponsor: University of Maryland, College Park – NIH
Harnessing Biomaterials to Study the Link Between Local Lymph Node Function and Systemic Tolerance
This proposal combines the advantages of biomaterials (e.g., co-delivery of multiple signals, controlled release) with direct LN injection for the first time to study the link between local LN function and systemic tolerance. Our in vivo studies demonstrate that a single treatment with myelin antigen (MOG)/rapamycin immunosuppression (rapa) depots permanently reverses disease and paralysis in mouse models of multiple sclerosis (EAE), even when depots are administered at the peak of disease to non-draining LNs. Thus, a treatment given during the peak of inflammation and remote from the inflammatory site is curative. Our overarching goal is to dissect the role of signal location, combination, and kinetics on the structure and function of LNs, and reveal how these local changes bias the degree and specificity of tolerance in other lymphoid organs, at disease sites (i.e., CNS), and systemically.
Sponsor: University of Maryland, College Park – NIH
Improving Multiple Sclerosis Patient Quality of Life Using Microneedle Patches to Simplify Delivery of MS Drugs
New findings indicate co-administration of regulatory signals with self-antigens can promote tolerogenic responses against antigens, instead of inflammation. We will develop a simple, modular system that mimics attractive features of biomaterials (e.g., co-delivery, tunable cargo loading), but built entirely from immune signals. These structures—termed immune polyelectrolyte multilayers (iPEMs)—are assembled by electrostatic interaction of self-peptides linked to cationic amino acids, and regulatory nucleic acid TLR ligands (anionic). iPEMs will be assembled on unique microneedle arrays that eliminate needles, stabilize cargo, and efficiently penetrate skin to deliver iPEMs to skin-resident dendritic cells (DCs). This idea offers transformative potential by addressing three key challenges hindering autoimmune therapies: 1) intrinsic inflammatory features of biomaterials that could exacerbate disease, 2) poor control over the signals and context in which DCs encounter self-antigen, and 3) lack of specificity of current treatments that leave patients immunocompromised. The project will employ tools from nanotechnology and immunology, leveraging self assembly, transgenic animals, and testing in human multiple sclerosis patient samples and mouse models of multiple sclerosis and type 1 diabetes.
Sponsor: University of Maryland, College Park – NIH
Tunable Assembly of Regulatory Immune Signals to Promote Myelin-Specific Tolerance
Strategies that mimic attractive features of biomaterials, while eliminating inflammatory “carrier” effects could be transformative for new therapies for autoimmune diseases. Toward this goal, the proposed research will use polyionic immune signals to create novel nanostructured capsules built entirely from regulatory immune signals and myelin antigens. These immune polyelectrolyte multilayers (“iPEMs”) are assembled through electrostatic interactions on a template, which is then removed to leave vaccines capsules that juxtapose myelin and Toll-like Receptor (TLR9)-suppressive nucleic acids (GpG). Since there is no carrier, the density of signals in iPEMs is very high relative to lipid or polymer formulations with cargo embedded in a matrix. The proposed work will build on these findings to test the hypotheses that assembly of self-antigen and regulatory immune signals generates tolerance in mouse models of multiple sclerosis. VA support for this project could enable technology that creates more specific and effective treatments for multiple sclerosis or other autoimmune diseases that impact many Veterans.
Sponsor: University of Maryland, College Park – VA
III. Clinical and Translational Studies in Renal Transplantation
Non Invasive Blood Test to Diagnose Acute Rejection After Pancreas and Kidney Transplantation: Pancreas and Renal Rejection Diagnosis Using Circulating Donor-Derived Cell-free DNA in Peripheral Blood
Donor-derived cell free DNA (dd-cfDNA) has shown promise as an early marker for cellular injury caused by rejection. dd-cfDNA changes may also indicate other injuries that lead to progressive decline in transplant organ function. This is an investigator initiated study, where we have chosen to study donor-derived cell-free DNA analyzed by the clinical laboratory at CareDx in Brisbane, CA. The CareDx dd-cfDNA test measures the amount of circulating donor-derived cfDNA as a percentage of total cfDNA in transplant recipients. After isolating cfDNA from blood collected in the Streck Cell-Free DNA BCT tube, regions including highly variable single nucleotide polymorphism (SNP) sites will be analyzed. Next-generation sequencing will be used to calculate the frequency of donor allele at each site, and the fraction of dd-cfDNA will be calculated using the CareDx proprietary algorithm. The dd-cfDNA measurement is intended for the quantitative detection of plasma dd-cfDNA as a % of the total plasma cell-free DNA.
Sponsor: CareDx, Inc
Assessment and Significance Allograft Rejection in Kidney Transplantation Using HistoMap and Formalin Fixed Paraffin Embedded Tissue
Both clinical and experimental observations suggest that allograft rejection is a complex process with multiple components that are, at least partially, functionally redundant. To investigate this complex process, oligonucleotide microarrays have been used to generate quantitative mRNA expression profiles following transplantation. Patterns of gene expression have been confirmed with real-time PCR data, showing a hierarchical clustering algorithms clearly differentiated the early and late phases of rejection. The NanoString nCounter Gene Expression Assay, a robust and highly reproducible method for detecting the expression of up 770 genes in a single reaction with high sensitivity and linearity across a broad range of expression levels. The methodology serves to bridge the gap between genome-wide (microarrays) and targeted (real-time quantitative PCR) expression profiling. HistoMap is based on direct digital detection of mRNA molecules of interest using target-specific, color-coded probe pairs. The HistoMap panel has been developed specifically for use with the predominant transplant organs including kidney, heart, lung and liver and includes genes across 37 different pathways, critical components of the immune response, tissue injury and mechanisms of action for immunosuppressive drugs. The objective of this study is to use retrospective samples from transplant kidney biopsies that show allograft rejection to validate the nCounter platform.
Sponsor: CareDx, Inc.
Innate B Cell Immunity and Antibody-Mediated Rejection of Human Kidney Allografts
The goal of the present study is to further investigate the role of Nabs IgG in the outcome of kidney transplants in a large group of patients treated at multiple centers. Our main objective is to assess the value of serum IgG Nabs as a biomarker for rejection (ABMR) and ultimately graft loss following kidney transplantation. We will also examine whether the development of IgG Nabs correlate with anti-HLA antibodies and DSA.
Sponsor: Trustees of Columbia Univ in the City of New York – Medical – NIH
The Prospera Kidney Transplant ACTIVE Rejection Assessment Registry (Proactive) Study
The ProActive registry is a longitudinal, multi-center study with a prospective arm observing clinical care for patients receiving physician-ordered Prospera, an allograft rejection test, and a historical control arm collecting data on cases at the same sites who had kidney allograft rejection managed with SCr/eGFR. This registry will compare patient management and outcomes in patients who receive Prospera (Prospera arm) to the outcomes of the historical control group (control arm) to determine Prospera’s clinical utility. The PROSPERA™ test detects allograft rejection noninvasively and with high accuracy, by measuring the fraction of dd-cfDNA in the patient’s blood, without the need for prior donor or recipient genotyping.
Sponsor: Natera, Inc.
U Maryland Mid-Atlantic APOLLO Research Network Omic and Clinical Center
Prospective, observational cohort study to genotype all African-American living and deceased donor kidneys for APOL1 risk variants, and correlate genotype with allograft outcomes: trajectory of allograft function, graft survival, T cell and B cell mediated acute rejection. An associated objective is to estimate the trajectory of native kidney function, blood pressure, and albuminuria among living kidney donors in relation to APOL1 genotype.
Sponsor: NIH-National Institutes of Health
Evaluation of Patient Outcomes from the Kidney Allograft Outcomes AlloSure Registry (KOAR)
This is a multicenter, non-blinded, prospective observational cohort study of 1000 patients enrolled in an AlloSure testing registry, including 300 patients at centers with planned renal surveillance biopsies at 12 months post-transplantation. The other 700 patients will be from centers that do not perform protocol surveillance biopsies. This registry study does not provide any medical care. Outcomes in this sub-cohort, which represents the majority of the intended use population in the U.S., will be compared to the outcomes of the test and control cohorts. A matched control cohort of 300 patients will be retrospectively selected from the subset of centers providing the test cohort patients who have planned surveillance biopsies at 12 months post-transplant. The primary safety objective is to test the hypothesis that a strategy of monitoring for rejection that introduces AlloSure® into clinical practice does not lead to inferior renal allograft outcomes when compared to a strategy of monitoring for rejection that does not include AlloSure. The primary efficacy objective is to test the hypothesis that a strategy of monitoring for rejection that introduces AlloSure into clinical practice results in a reduction in the number of renal biopsies performed when compared to a strategy of clinical care without the use of AlloSure.
Sponsor: CareDx, Inc.
Laboratory Members
