 What are Chest Wall deformities?
What are Chest Wall deformities?
Conditions affecting the chest wall can either be congenital or developmental (occurring naturally as part of growth) or acquired secondary to other conditions such as surgery or trauma. The University of Maryland Chest Wall Deformity clinic will see and treat both conditions.
Common developmental chest wall deformities include Pectus Carinatum, sometimes called pigeon breast or pigeon chest, congenital or acquired Jeune Syndrome (or narrow chest) as well as Pectus Excavatum (funnel chest).
What is pectus carinatum?
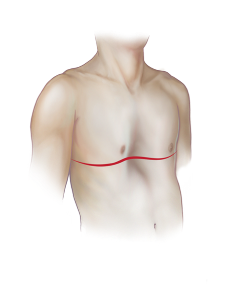
Pectus carinatum is a deformity of the chest wall in which the breastbone and ribs are pushed outward. Pectus carinatum is sometimes called “pigeon breast” because of the birdlike appearance of the chest. The condition occurs in about 1 out of 1,000 with males more frequently affected than females.
While surgical repair is an option this condition can often be treated by a prosthetic brace. Severe conditions can be treated by surgical repair.
What is Jeune Syndrome?
Jeune's Syndrome is a form of congenital deformity of their chest wall where the chest cage is extremely small and doesn't have enough room for proper breathing. The ribs are broad, short and irregularly joined between the cartilage and sternum, or breastbone. This produces a bell-shaped, inflexible chest cavity, which doesn't grow well in time.
In addition to such congenital cases acquired Jeune’s syndrome can occur due to childhood trauma or surgically induced alterations in chest wall growth resulting from childhood repair. University of Maryland Surgeons have experience in treating adults with acquired Jeune syndrome although the majority of these cases are treated in childhood.
 What is pectus excavatum?
What is pectus excavatum?
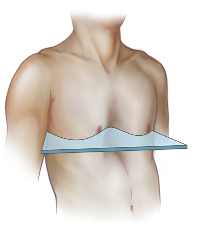
Pectus excavatum is a congenital deformity of the bones and cartilage of the chest where several ribs and the breastbone (sternum) grow in an inward direction resulting in a sunken appearance of the center of the chest. It is sometimes called “funnel chest” and usually involves the lower half of the sternum. It is associated with "flaring" of the lower ribs accentuating the appearance of the depth of the depression. While most common in the middle of the chest, it may move to one side, which is typically on the right.
What causes pectus excavatum?
While no one knows exactly what causes pectus excavatum, most people with the condition have had it since birth or early infancy and it is found to run in families. It may occur because of uncoordinated growth between the cartilage at the end of the ribs and the chest.
If the cartilage is growing faster than the expansion of the heart and lungs, which pushing the sternum outward, then the sternum will be pushed inward. Once this occurs, the deformity either persists or gets worse.
What are the symptoms of pectus excavatum?
Severe pectus excavatum causes a deep hollow in the chest that can put pressure on the lungs and heart, causing:
- Chest pain
- Decreased exercise tolerance
- Easily fatigued
- Limitations with physical activities
- Coughing or wheezing
How is pectus excavatum diagnosed?
A physical exam and a detailed medical history are performed by a doctor to determine what symptoms may be attributable to the defect. In addition, specialized tests are often required to determine who should be offered surgical treatment and check for any other associated medical conditions.
Routine tests for adults include:
- X-ray, CT or MRI scan of chest
- echocardiogram to test heart function
- pulmonary function tests to check lung volume
- exercise stress testing to measure exercise tolerance
What are the treatment options?
Non-Surgical
Despite at times severe deformity it is possible to have no physiologic side effects. If that is the case our team will monitor your condition and repair only if it becomes necessary
Surgical Repair
 Ravitch Procedure: This procedure is the original one developed for repair of pectus excavatum. It is associated with the best and longest lasting results, improvement in symptoms and long-term patient satisfaction, but it does require a larger incision in the middle of the chest. The operation involves removal of the ends of the ribs (known as the cartilage) as they attach to the sternum in the depressed area.
Ravitch Procedure: This procedure is the original one developed for repair of pectus excavatum. It is associated with the best and longest lasting results, improvement in symptoms and long-term patient satisfaction, but it does require a larger incision in the middle of the chest. The operation involves removal of the ends of the ribs (known as the cartilage) as they attach to the sternum in the depressed area.
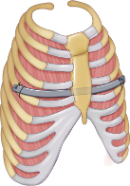
The lining membrane around the rib (known as the perichondrium) is left in place. The sternum is then straightened out at the point where it turns downward and held in this position using stitches. The chest is then properly adjusted and put into place using a metal bar or strut that goes under the sternum to keep it in an outward position. The bar is removed after one year after the chest heals in place.
- Physicians at the University of Maryland tend to perform a modified Ravitch procedure which removes a smaller portion of the cartilage but still produces similar results
- Average hospital stay is two to three days
- Despite the bigger incision pain is well controlled with oral medications and operation results in pain levels similar to any other chest operation
- Nuss Procedure: Also known as Minimally Invasive Repair of Pectus Excavatum (MIRPE), has the advantages of smaller incisions on the side of the chest rather than the middle, avoidance of cartilage or bone removal. This operation has proved popular and successful in the pediatric population as the chest wall has not yet developed the rigidity associated with the adult rib cage.
This procedure may be appropriate for some, but not all adult patients. The Nuss procedure in adults requires modifications and often more than one Nuss bar are required to address the repair and each bar is recommended to remain in place for a minimum of 2 years.- Average hospital stay is two to three days
- Bar removal is performed in a separate short operation that does not require another hospitalization.


What is the best operation for pectus excavatum?
The Nuss procedure offers the ability to return to normal activities sooner as the chest wall is still intact but sometimes pain can be an issue. The ribs must grow back for complete chest wall stability with the Ravitch procedure, which may take a few months to happen. The likelihood of recurrence of chest deformity after the Nuss procedure has been slightly greater than that of the Ravitch procedure. With either procedure normal work related activity and non-contact sports can be resumed after a few months but contact sports must be avoided until the bar is removed. Your surgeon will help you determine which treatment is best for you.
 Contact us for more information
Contact us for more information
410-328-6366
Alexander Krupnick, MD is director of the Adult Pectus Excavatum Clinic